BACKGROUND
Cambodia’s development trends are moving toward lifestyle and food consumption changes which are leading to increased risks for Non-Communicable Diseases (NCDs), including in rural areas.
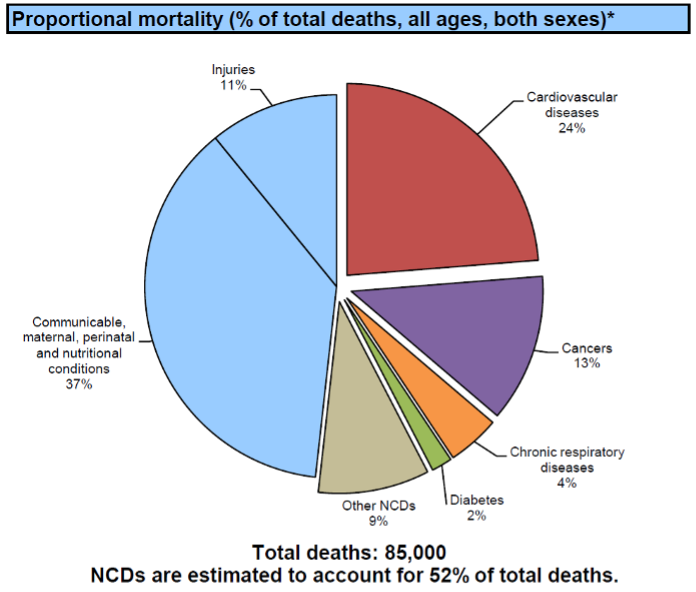
Cardiovascular disease, cancer, chronic respiratory disease, and diabetes alone cause 46%of deaths in Cambodia. NCDs are affecting Cambodians in their productive years. As an indicator of trends, obesity increased from 15.4% to 21.9% from 2010 to 2016 and continues to rise.
Community members in ADRA’s rural Bakan District expressed that medical costs to manage NCDs are increasingly utilizing family financial resources. Local health departments are focused on medicine-based management, but this is often only provided by a mobile team instead of being available at local health centers.
NCD impacts are most experienced by older child caregivers who are at home while their children are working away from the home or have migrated to distant areas leaving their children with their grandparents. Health destructive tobacco and alcohol, with their associated negative health and social impacts, also compete for limited household resources leading to increased poverty.
INTERVENTION
Following years of addressing tobacco issues in Cambodia, beginning in 2015 ADRA Cambodia began addressing broader lifestyle health issues with a NCD Lifestyle Health promotion program called “LiveMore” which is contextualized from the CHIP (Complete Health Improvement Program) model, in rural villages.
In 2020, ADRA Cambodia’s Best CHOICES project, an ANCP Australia program, began promoting the “LiveMore” model in 24 villages, including advocacy with and training of Ministry of Health (MOH) officials at all levels. Following this training, the model trains community-based facilitators who then conduct participatory self-help behavior change sessions in their village.

The MOH Health Center staff and these community -based facilitators work with the project to conduct community wide risk assessments focusing on identifying persons with high blood pressure, high blood glucose levels, obesity/high BMI (body mass index), or other known risks.
Villages observed with risk factors are encouraged to join the 18 LiveMore sessions. The behaviour change session groups meet starting bi-weekly and then weekly over a 3-month period. Collection of biometric/blood testing is conducted at day 0, 30, and 90 together with the lifestyle health behavior information for analysis and sharing of feedback to participants for motivation.
The sessions begin with discussions on chronic disease, lifestyle medicine and the optimal lifestyle and cover specific NCDs and behavior motivations. Complimentary health issues are addressed for child caregivers as well as others in the target communities facing risks to Non-Communicable Diseases.
Between 2020 and 2022, the project conducted lifestyle health pre-screening sessions in 24 communities. 446 community members (300 females, 146 males), identified as “at-risk” due to high blood-glucose, high blood pressure, or elevated body-mass-index (BMI), were invited to join a lifestyle change group. Majority of group members were between the ages of 35 and 70 years of age.
Key results for the participants as measured between Day 0 to Day 90 include:
- 64% of the 255 participants with elevated high blood pressure were able to lower their systolic blood pressure.
- 77% of participants with LDL (low-density lipoprotein) cholesterol over 130 were able to reduce this risk factor and 61% with elevated (>150) levels were able to reduce their triglyceride levels.
The program marked changes in lifestyle of at-risk members with key results as follows:
- Elevated usage of salt was reduced from 98% to 77% and usage of beans and nuts was increased from 54% to 77%.
- The use of coffee was reduced from 22% to 14% consuming coffee 2 or more times per week. – Quitting the use of alcoholic beverages was strongly encouraged with 50% of those who drank making this key change.
- Physical activity levels showed an increase from 76% to 95% of participants having physical activity at least 5 times per week.
As Cambodia’s lifestyle and food consumption changes continue to lead to increased risk of NCDs, ADRA Cambodia is committed to continuing interventions to support those at risk. This is achieved by using results to actively engage in forums at the local levels and national stage to promote lifestyle health programs and seek national policies within the Ministry of Health and national government to protect the lives and wellbeing of those at risk.
Authors: Mark & Ann Schwisow, ADRA Cambodia
Photo: © 2022 | ADRA Cambodia
*This article was featured under ‘Technical Focus’ in ADRA Asia Regional Office’s quarterly Magazine ADRA Asia Focus Vol 2 | No 3*
Visit the ADRA Cambodia website to learn more: https://adracambodia.org/